Correcting problems in hair restoration surgery: an update
|
|
|
- Jerome Barton
- 6 years ago
- Views:
Transcription
1 Facial Plast Surg Clin N Am 12 (2004) Correcting problems in hair restoration surgery: an update James E. Vogel, MD, FACS Division of Plastic Surgery, Johns Hopkins School of Medicine and Hospital, 1838 Greene Tree Road, Suite 420, Baltimore, MD 21208, USA address: jevps@comcast.net The techniques of hair restoration surgery have advanced particularly rapidly over the past two decades. These advances have achieved a current standard that allows-natural appearing surgical hair restoration that does not provide visual evidence to the casual observer that a surgical procedure was performed [1 4]. The standards of surgical care in previous years could not provide this same advantage to patients [5]. Today there remain a variety of unnatural surgical hair transplant results in patients whose procedures were performed using older techniques. These patients often bear the physical and emotional scars of an unnatural hair appearance and harbor a distrust for the field of hair restoration surgery and its surgical practitioners. The challenge for the hair restoration surgeon is to provide a level of expertise and honesty to these unfortunate patients to restore their appearance and self-confidence. The purpose of this article is to describe the most commonly seen problems in clinical practice and describe a practical approach to their correction. The majority of patient complaints seen clinically concern a straight, pluggy, or cornrow appearance of grafts or the malposition of their anterior hairline. Patients also frequently complain about the progression of the their own baldness and the resulting separation of the previous transplants from the receding hairline. In the majority of patients a clinically significant improvement in appearance can be achieved after one corrective procedure; however, as a general rule two or more staged operations are needed to maximally improve the results of previous hair restoration procedures. The techniques of anesthesia, scalp preparation, and instrumentation have be published and reviewed elsewhere [6,7]. Correcting cornrow plugs at the anterior hairline and crown-vertex area The appearance of rows of hair plugs resembles a cornfield, thus the commonly used term cornrow hair transplant. The first person to describe a technique for improving this unnatural plug appearance was Lucas [8]. Others have modified this original technique and described other approaches to correcting previous unsightly hair transplant results [9 13]. The original description by Lucas was to partially excise the plugs using a 1.5- to 1.7-mm punch biopsy instrument. His original description was to allow these small circular wounds to heal secondarily. It is preferable to close these circular wounds because of annoying serous seepage from the open sites and the delay in separation of the plug reduction site eschar. The current approach is to close the wounds, primarily with a 3-0 chromic suture (Fig. 1). In general, the current approach to correcting the plugs at the anterior hairline involves performing plug reduction and recycling (PR&R). The technical details of the procedure have been detailed previously [9]. This procedure is aggressively applied to at least the anterior two rows of plugs. In general, during the first corrective session every other plug in a row can be selected for PR&R. The plugs to be reduced are selected and trimmed to a length of approximately 3 mm. A punch biopsy tool that is the same size of the plug or slightly smaller is selected. For example, the typical size for a traditional plug is 4 mm, so a 3.75-mm punch biopsy would be selected for the plug reduction. Using a smaller punch size would leave /04/$ see front matter D 2004 Elsevier Inc. All rights reserved. doi: /j.fsc
 Punch excision sites are closed with chromic suture.")
2 264 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) Fig. 1. Technique of plug reduction. (A) Alternating plug transplants are trimmed to 3 mm. (B) 3.75-mm biopsy punches are made into 4-mm plugs, which leaves some small grafts. (C) Punch excision sites are closed with chromic suture. (D) Recycled hairs from the removed punches are prepared into one- and two-hair grafts and transplanted around the plug reduction sites to recreate the hairline. too much residual plug and incompletely treat the clumped and often compressed plug appearance. The punch is positioned eccentrically to leave a crescent shape of the remaining original plug, which effectively leaves behind a linear graft of approximately three to four hairs. The recycled hair and the additional hair harvested from the occipital region are densely transplanted anterior and posterior to the plug reduction sites. Usually several wide tracks of alopecia exist between the linear rows of plugs, which need to be densely transplanted. Plugs that exist more than 2.5 to 3 cm posterior to the anterior hairline can generally be left intact. Aggressive management of the first two or three rows of plugs as described is usually all that is needed to soften and camouflage the leading edge of cornrow-appearing grafts. In this way the density of the plugs posteriorly (the only redeeming quality of large, circular grafts) can be combined with the soft look of the anterior hairline zone. When removing the plug it is important to angle the punch parallel to the follicles. Reducing the number of transected hairs in the resected plug maximizes the recycling yield. Care should also be taken to pass the punch instrument deep enough to include 1 to 2 mm of subpapillary fat. Including the entire papilla and its underlying fat accomplishes two goals: (1) removal of the entire plug papilla increases the likelihood of no regrowth of the original in situ hair, and (2) sufficient fat below the intact hair follicle helps to maintain viability of the grafts as they are trimmed and recycled. The use of sharp excision punches and frequent exchange of a punch when it becomes dull is also an important technical point to minimize shearing and damage to the peripheral plug follicles. Accurate assessment of the hair restoration problem is the key to designing the best possible solution for the patient. It is important to determine the objective problems of the previous procedures and to integrate the chief complaints of the patient. For example, the patient might be primarily concerned with the pluggy appearance in the crown area but not terribly unhappy with the hairline appearance. In this



 was a 28-year-old man who underwent two sessions of 4-mm plug grafts at an earlier age. The grafts were interspersed with his existing hair, which had been progressively lost over the last 5 years.")
3 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) case, the surgical priority and the use of valuable and limited donor hair needs to be focused in the crown region. Because hair loss follows typical patterns according to the Norwood classification scheme, repetitive scenarios of problems from past transplants frequently appear. The cases that follow are presented to illustrate a series of different types of problems. They are presented as progressively more complex cases of repair. For purposes of organization, the levels of complexity for repair are categorized as minimal, moderate, orextreme. Minimally complex scenarios The first two cases illustrate situations that are relatively straightforward to repair. These cases and ones similar to them can usually be corrected to an acceptable level with two procedures. The three most important features that render these cases minimally complex to repair are: 1. relatively high position of the hairlines 2. minimal to moderate nature of the plug intensity 3. moderately plentiful donor hair supply in the occipital scalp Case 1 Case 1 (Fig. 2) was a 28-year-old man who underwent two sessions of 4-mm plug grafts at an earlier age. The grafts were interspersed with his existing hair, which had been progressively lost over the last 5 years. His exposed plugs were located at 9 cm from the glabela. Because of the height of the plug hairline, a straightforward procedure of PR&R could be performed. In addition to the recycled hair, 1200 grafts were harvested from the occipital donor Fig. 2. Case 1: minimally complex scenario. (A) Pre- and intraoperative appearance following the first session of PR&R. (B D) Results at 1 year following the last procedure. Two sessions of PR&R plus 1200 grafts were performed.
 was a 33-year-old man whose straight line of plug grafts was exposed prominently with progressive loss of the frontal tuft he had when the plugs were planted.")


4 266 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) area and grafted in the anterior hairline. In two sessions the patient s hairline was acceptable. Case 2 Case 2 (Fig. 3) was a 33-year-old man whose straight line of plug grafts was exposed prominently with progressive loss of the frontal tuft he had when the plugs were planted. The best approach for this patient was also a PR&R procedure because of the high position of his hairline and the relatively plentiful supply of donor hair. In addition to the recycled hair, 1800 grafts were harvested from the occipital donor area and grafted into the anterior hairline. Although Case 2 s hairline was more intense than Case 1 s hairline (see Fig. 2), two sessions of PR&R and a greater number of grafts were needed. Moderately complex scenarios The next two cases illustrate situations that are relatively more difficult to repair. These cases and ones similar to them can usually be corrected to an acceptable level with three procedures. The four most important features that render these cases moderately complex to repair are: 1. intensely pluggy hairlines caused by creation of a wall of grafts 2. relatively coarse hair texture that creates an even more solid hairline appearance 3. moderate depletion of donor hair supply in the occipital scalp 4. problematic plug grafts in the crown-vertex area An important common thread to the planning of the next three cases is the simultaneous corrective repair in the frontal and crown area. Surgically appropriate aggressive planning and execution is essential to complete the repair in as few procedures as possible. Patients certainly appreciate this approach because they are naturally frustrated with their current hair appearance. In addition, recovery from simulta- Fig. 3. Case 2: minimally complex scenario. (A C) Pre- and postoperative appearance following two sessions of PR&R plus 1800 grafts. Results are seen 1 year following his last procedure.





5 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) neous frontal and crown surgery is not generally prolonged compared with surgery on a single site. Case 3 Case 3 (Fig. 4) was a 56-year-old man who wore a hairpiece to hide the unnatural appearance of his previous transplant and progressive hair loss. Because the hairline was at a reasonable height and the sharp hairline did not cross the midline, the plan for PR&R was acceptable. Another option would have been direct and total excision of the entire anterior hairline, including the nongrafted forehead Fig. 4. Case 3: moderately complex scenario. (A) Anterior hairline appearance, preoperative appearance, first session intraoperatively, results following first session, and two sessions intraoperatively. (B) Crown-vertex appearance, preoperative appearance, first session intraoperatively, results following first session, and two sessions intraoperatively. (C E) Results following the third session of PR&R plus 2000 grafts. The results are seen 1.5 years following the last procedure.



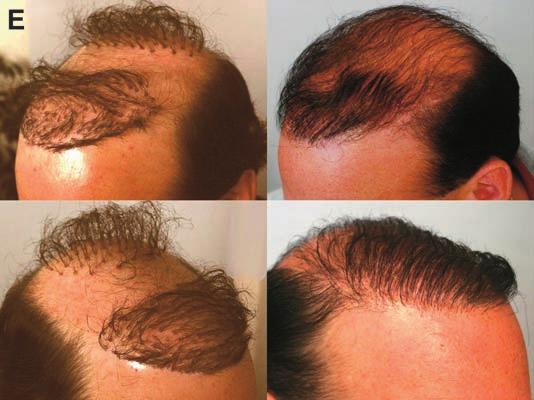
6 268 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) scalp. Case 3 underwent three sessions of PR&R to the anterior hairline and crown-vertex area. He also had 2000 grafts transplanted to the hairline, forelock, and crown-vertex area. Cases 4 and 5 Cases 4 and 5 (Figs. 5, 6) were two men in their mid-40s whose coarse hair rendered the pluggy hairline an intense wall of hair. It took four sessions to soften the intense frontal line of hair and eliminate the plugginess of their crown grafts. Both patients underwent PR&R and approximately 1500 grafts at the anterior hairline and crown-vertex area. Both patients underwent their procedures before linear excision of hairline grafts was recommended more frequently. The linear excision technique would have expedited the completion of the repair and eliminated one or two plug reduction sessions. The fact that two patients can be grouped together in one similar description and plan underscores the common theme of their problem. The chief problem they shared was the coarse nature of their donor hair, which produced an intense wall at the hairline. These grafts were performed at an early age in the crown and hairline areas only to be later exposed dramatically by progressive hair loss. Case 6 Case 6 (Fig. 7) was the most challenging case to repair in this group. This 43-year-old man had a hairline that was at a good height (~8.5 9 cm), but Fig. 5. Case 4: moderately complex scenario. (A) Anterior hairline appearance, preoperative appearance, first session intraoperatively, results following first session, and two sessions intraoperatively. (B, C) Results following fourth session of PR&R plus approximately 1500 grafts. Results are seen 1 year following the last session. Linear excision of the hairline plugs would have expedited the corrective process.
 Anterior hairline and crown-vertex appearance preoperatively, and appearance and first session intraoperatively.")


7 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) Fig. 6. Case 5: moderately complex scenario. (A) Anterior hairline and crown-vertex appearance preoperatively, and appearance and first session intraoperatively. (B, C) Results following fourth session of PR&R plus approximately 1500 grafts to anterior hairline and crown-vertex area. Note the change in hair color, which by virtue of diminished contrast between hair and scalp also renders the appearance more natural. Linear excision of the hairline plugs would have expedited the corrective process. it was straight and pluggy-appearing. He had unsightly plug grafts in the crown area and minimal donor hair in the occipital area. The quality of his donor hair was also thin with a silky texture. These donor qualities rendered the hair less suitable for camouflaging the scalp and the unsightly grafts. The emergence of the round, pencil-sized scars from previous plug harvest sites were also beginning to show through his thinning occipital donor area. Given these preoperative assessments, a direct and aggressive attack on the anterior hairline was planned. A linear excision of the entire hairline was performed with recycling of these plug grafts into follicular units that were regrafted anterior to the hairline excision closure site. Simultaneously, the crown plugs were treated with PR&R. In the two subsequent procedures, small grafting sessions of 600 grafts each were performed to the hairline, forelock, and crown region alongwithplugreductionsinselectedareas.the principal advantage of the direct linear excision in this case was (1) a focused assault on the unsightly plug hairline with rapid improvement in its visual unsightliness, and (2) procurement of moderate donor supply in the setting of limited occipital hair availability. Correcting problems of hairline design The correct design of an anterior hairline is of equal importance to the use of hair grafts that are

 Intraoperative excision outline, actual hairline excision specimen, appearance following")
.")
 Results following third session (one linear excision and two PR&R plus f1200 grafts).")


8 270 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) Fig. 7. Case 6: moderately complex scenario. (A) Anterior hairline and crown-vertex appearance, preoperative appearance. (B) Intraoperative excision outline, actual hairline excision specimen, appearance following closure of the hairline excision wound, and recycled hair grafts placed in an irregular distribution (all during first session). (C) Intraoperative appearance of first and second sessions of PR&R in the crown-vertex area. (D F) Results following third session (one linear excision and two PR&R plus f1200 grafts). Results are seen about 1 year following the last procedure. natural and undetectable. Briefly, the hairline needs to be symmetric and exhibit bilateral temporal recessions. A mature man s hairline is usually not less than 8.0 to 8.5 cm from the midglabela area. The most common problems associated with hairline design are blunted temporal angles or hairlines placed too low on the forehead. The combined use of modified forehead lifting, scalp reduction, hair grafting, and plug reductions can result in a satisfactory improvement in patients who have problems with hairline design.





9 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) Fig. 8. Case 7: extremely complex scenario. (A, B) Preoperative appearance of low positioned, pluggy grafts that became isolated from the remaining hairline as a result of progressive hair loss. (C) Intraoperative appearance of first session of linear excision of entire anterior hairline and front three rows of plugs with recycling and second session of PR&R. (D, E) Result following third session of grafting alone plus 3000 grafts. Results seen are approximately 1 year following the last procedure. Extremely complex scenarios The next two cases illustrate situations that are among the most challenging to repair. The four most important features that often coexist that render problems of hairline design extremely complex to repair are: 1. hairline placement too low to be maintained for achieving a natural appearance
10 272 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) extreme progression of hair loss that renders the current appearance most unusual 3. extreme depletion of hair in the occipital donor sites 4. moderate to considerable scarring in the scalp with poor mobility Case 7 Case 7 (Fig. 8) was a 57-year-old patient who underwent isolated plug grafts at an early age when he had minimal hair loss in the temporal areas. With progression of hair loss he developed a devilish distribution of his temporal hair grafts. To camouflage this appearance he had a tight perm applied to his hair and chose a hairstyle similar to a loose afro. The level of the grafts was approximately 6 cm from the glabela. This low placement of the plugs rendered the surgical alternative of plug reduction and grafting within and anterior to the plugs a nonoption. Fortunately there was excellent scalp and forehead mobility and a good supply of donor hair available. He underwent a series of three procedures. The first procedure was a linear excision of the front three rows of the temporal plugs. The excision pattern extended across the entire forehead to avoid dog-ear deformities that would occur at either end of the temporal ellipses. At the first session he also received 1200 grafts to the anterior hairline and forelock area. The recycled temporal grafts and newly harvested donor hair served as the source for the grafts. He subsequently underwent two additional procedures with 3000 grafts to the hairline and forelock and crown area along with PR&R of the remaining plugs not originally excised in the temporal area. In this case the benefits of the linear excision were those mentioned in Case 6 (see Fig. 7) and the ability to elevate the hairline. Elevation of the hairline is a key benefit to linear excision because it allows for robust grafting at an appropriate hairline level. The opportunity to graft 0.5 to 1 cm below the linear excision scar hides the linear excision scar and creates a soft transition at the hairline. Case 8 Case 8 (Fig. 9) was a 30-year-old man who had undergone transplantation with 3-mm and 4-mm plugs at age 19. With progressive alopecia his plugs became more noticeable. The plugs also became progressively isolated from his receding hairline. The isolation of the hair grafts resulted in an alley of alopecia between his anterior hairline grafts and the receded temporal fringe. The plug hairline was also too low (7 cm from the glabela). Prominent and unsightly 4-mm plug grafts also pocked his crown-vertex area. The progressive hair loss between his frontal and crown areas resulted in a bizarre appearance. He had minimal donor hair available in the occipital area and his scalp was moderately tight because of scarring from anteriorly and posteriorly placed grafts. The following were the requirements for this patient s surgical repair: 1. elevation of the anterior hairline 2. reduction of the temporal alleys 3. softening of the anterior hairline plugs 4. elimination of the crown-vertex plugs 5. creation of a natural forelock distribution of grafts The first procedure was performance of an M-shaped scalp reduction originally described by Marzola [14]. The M pattern has several advantages. First, all scars left from the excision fall within the zone of a forelock distribution and can be covered with subsequent grafting. Second, the M design permits maximum flexibility with regard to which flaps can be elevated and advanced. In Case 8 the anterior and two temporal flaps were advanced. This advancement accomplished hairline elevation with concomitant plug excision and raised the temporal fringe while eliminating the alleys of alopecia. During the first operation and in a series of three additional procedures, extensive plug reductions were performed in the crown, vertex, and forelock area. A total of 1800 grafts were ultimately transplanted with the donor hair originating from occipital donor harvest and plug recycling. Correcting problems in the donor harvest site Donor site scarring is an absolute consequence following a transplant. The scars can range from im- Fig. 9. Case 8: extremely complex scenario. (A) Preoperative appearance of low pluggy hairline, temporal alleys of alopecia, isolated crown-vertex plugs, and considerable intervening alopecia. (B) Intraoperative outline of M-shaped scalp reduction pattern and immediate on-table result following the scalp reduction and recycling of hair grafts. (C) Numerous sessions of plug reductions were performed in the frontal and crown-vertex areas. (D, E) Results following five procedures over a 2.5-year period. A normal forelock pattern is established. Note the heightened self-esteem that is seen in the patient s eyes postoperatively.




11 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004)

12 274 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) perceptible to extremely deforming. The corrective approach depends on the following features. 1. objective size and subjective concern of scar deformity 2. laxity of the surrounding occipital scalp 3. vascular integrity of the surrounding scalp 4. degree of current hair loss and prognosis for future loss 5. shift or alteration of surrounding donor hair level 6. preferred hairstyle Case 9 Case 9 (Fig. 10) was a patient who had a commonly seen donor scar problem that was approximately 1.5 cm wide. It had occurred because of multiple (two or three) donor harvest procedures in the same area with considerable residual tension on the closure line. Despite this, the surrounding scalp still had some suitable mobility. A running W-plasty was performed as a single stage procedure at the time of reharvesting for an additional transplant. In this procedure the peak on one side of the incision interdigitates into the valley on the contralateral side. Closure in this case was accomplished with minimal tension after some moderate wound edge undermining. Numerous permanent sutures were used in the deep layers to minimize wound edge separation postoperatively. The rationale for the W-plasty technique is twofold. First, it breaks up the linear nature of the scar and varies the direction of contractile forces during healing, thereby reducing recurrent scar widening. Second, it creates overlapping regions of scar alopecia with hair-bearing scalp. Some scar alopecia will inevitably remain, however, and the shingling effect of the irregular closure enhances scalp and scar camouflage. Other forms of irregular pattern excision such as a Z-plasty or Frechet s triple flap [6,7] are based on the same premise, and these techniques can be used as indicated. Fig. 10. Case 9. (A, B) 1.5-cm scar in donor area following numerous harvest procedures in the same site. Outline of running W- plasty excision and repair is seen. (C) Intraoperative incisions before excision and repair of scar. (D) Interdigitated repair and closure.
 was a more dramatic example of overzealous harvest in the donor site.")




13 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) Case 10 Case 10 (Fig. 11) was a more dramatic example of overzealous harvest in the donor site. This patient underwent his third session of donor harvest in the same site. Although the skin edges were approximated, the vascular integrity of the scalp was sufficiently compromised with the tight closure that necrosis of the wound resulted. The most appropriate treatment in these situations was local wound care and Fig. 11. Case 10. (A, B) Wound necrosis with early and late healing by secondary intension after multiple overzealous harvests in the same donor area. (C) Rectangular tissue expander is placed in preparation for scalp advancement and excision of the scar. (D, E) Immediate and healed results following the procedure.

14 276 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) Fig. 12. Case 11. The result following 10 donor harvest procedures and two scalp reductions. From the standpoint of correcting the appearance of the donor area, no meaningful corrective surgery is possible. Camouflage techniques with hairstyle, a hairpiece, finasteride, and topical scalp coloring are the principal options. measures to promote healing by secondary intension. After 6 weeks of local wound care the edges epithelialized. An additional 8 weeks were needed for the surrounding tissue to soften sufficiently to assess the reconstructive options for this donor defect. Mobility was limited and there was no possible way to reapproximate the wound edges primarily or with a W-plasty. A tissue expander was the only realistic option for successfully obtaining sufficient mobility of surrounding scalp to permit excision of the scar and reapproximation of the wound edges. A rectangular expander was used, and after 10 weeks of inflation the scar was excised and closed. In retrospect, a W-plasty of the expanded flap should have been performed and would have likely produced an improved result. Patients expectations and the anticipated outcome must be carefully reviewed in all cases, especially when dealing with donor scar repairs. Case 11 Case 11 (Fig. 12) was an insoluble donor site problem. This unfortunate 31-year-old man underwent 10 transplants and two scalp reductions over a 10-year period. There is no viable surgical treatment to improve his donor scars. The adage of avoiding the problem initially as the best way to manage a complication is exemplified by this case. The only solution for this patient was to hide the donor scars. His options included growing his hair to a sufficient length then bundling it in a ponytail or wearing a hairpiece. Use of finasteride is also essential. Discussion The appearance of an individual who has the obvious cornrow hairline from older grafting techniques is a phenomenon known to most surgeons and lay people. The appearance is so striking and unfavorably memorable that most people know someone or have met someone who fits this description. It is not at all uncommon to hear a patient lament that his entire lifestyle revolves around the concealment of plugs. Frequently, patients who have unsightly plugs awaken early to devote the necessary morning hours
15 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) for hair grooming and cover-up. Often, individuals who have unnatural hair transplants plan social engagements in low-lit areas and avoid swimming or getting caught in the rain to avoid the obvious display of their hair plugs. In addition, these unfortunate patients who bear the burden of previous surgical misadventure are often devoted wearers of hats or hairpieces or resort to the perpetual use of scalp coloring creams or sprays. They often also carry the emotional burden of anger and distrust toward other hair transplant surgeons as a result of past experiences with hair restoration procedures. Thus, patients are incredibly grateful and their selfesteem and confidence is tremendously boosted when a technique is performed that reliably and safely eliminates the cornrows transplants, recycles the removed grafts, and improves the hairline. The techniques for correcting problem transplants continue to evolve. In the past 10 years the author and colleagues have performed approximately 500 corrective hair procedures on 200 patients. There have been no cases of scalp infection or postoperative hemorrhage in the donor or recipient area. In the patients receiving corrective transplants, the incidence of poor hair transplant growth, epidermal cysts, recipient scarring, and accelerated surrounding hair loss has been minimal, and no higher than in the author s patients receiving first-time transplants. The occipital donor sites in patients who have previously had punch harvesting of plugs that were left to heal by secondary intention are usually somewhat immobile and poorly vascularized, however. Some of the linear strip donor harvest scars used for corrective procedures have healed with greater scar widening than would have been expected in virgin occipital donor scalp, so the author and colleagues prefer to harvest longer, narrower donor strips when considerable donor scarring is present. When the plug reduction technique was first performed, the wounds were left open for closure by secondary intention. The current modification of the technique is to close these wounds primarily. Closure of the plug sites has been a welcome improvement for patients who have experienced both techniques. On the other hand, closure of the wounds creates two modest disadvantages from a surgical standpoint. First, multiple closures of the plug excision sites creates slightly more scalp tension in the region and can result in popping of newly planted grafts. Second, as a result of the popping and added scalp tension, grafts cannot be packed as closely to the plug reduction sites as when they are left open. These slight grafting disadvantages are a small trade-off for the accelerated healing of a closed wound and higher patient acceptance of the procedure. In some instances when extensive plug reductions are performed and grafting is planned in the local area, some plug reduction sites are left open to avoid excess tension on the scalp and to promote maximal take of the grafts. The procedure for excision of the linear strip of plugs at the hairline has numerous advantages. First, complete, direct excision of plugs translates into a focused attack on the unsightly hairline. Second, the excised strip of plugs represents a plentiful donor source for recycling of hair into grafts. Third, in cases in which the hairline is placed too low, linear excision of the plugs elevates the hairline. The advantage of the newly elevated hairline is a more balanced appearance and a larger space for grafting at the hairline to create a natural and irregular appearance. The efficiency of the direct linear excision of the hairline also expedites the entire corrective process. In most cases this technique will reduce at least one and sometimes a second procedure that would normally be expected following PR&R alone. Patients are often apprehensive about the prospect of the resultant scar following direct linear excision of anterior hairline plugs. The author and colleagues experience has been excellent with this technique from the standpoint of low visibility of the scar. A meticulous approximation of the wound edges, no tension on the closure, and extensive grafting into and around the scar has resulted in exceedingly high patient satisfaction with this approach. Another patient concern is the removal of previously transplanted hair, even if the grafts appear pluggy. Patients who have had transplants using older techniques often feel that they already have a shortage of hair and have paid a considerable price economically and physically going through a previous operation to obtain hair. Most patients accept the procedure of excision of plug grafts by any means when they are assured that the removed hair will be recycled and redistributed in other areas. Patients need to fully understand, however, that the recycling is not 100% efficient. The yield ranges from 50% to 85% following plug excision or linear excision and recycling into usable grafts. Finally, most patients accept the need for excision of plug grafts when they see photographs of hairlines that are incompletely corrected by grafting alone. The straight, pluggy hairline almost always requires an aggressive direct attack on the plugs. Other problems with older transplant techniques occur, including low density of grafts, poor graft survival, elevation or cobblestoning of grafts, misdirection of implantation angle, depression or pitting of grafts, necrosis of the scalp, and visible scarring around grafts. The problems most frequently seen in a
16 278 J.E. Vogel / Facial Plast Surg Clin N Am 12 (2004) clinical hair restoration practice and a practical approach to their correction are included in this article. Plugs placed in the crown-vertex are also well managed with PR&R. The main difference in managing plugs in this region is the determination of whether they should be removed entirely or simply reduced and the surrounding area grafted. The deciding factor is based on patient preference, the degree of crownvertex alopecia, and the amount of occipital donor supply. In cases in which plugs are to be removed and no additional grafting is planned, a punch size equal to or slightly larger than the plug should be used. When plugs are removed, the residual scar that remains in the crown alopecia can be imperceptible or can remain with variable degrees of prominence. Patients who request removal of plugs in the crown region need to be aware of the unpredictability of the plug excision scar. In most cases removal of the plugs with additional grafting is a more desirable option because the remaining plug excision scars are hidden well by the recycled grafts. When crown-vertex plugs are to be reduced and recycled, the eccentric plug excision technique is similar to that applied to the anterior hairline. Usually the most posterior 1 cm of plugs in this region are reduced, sutured, and recycled. Recycled plug grafts and newly harvested grafts from the occipital donor area are transplanted in areas of alopecia between the existing plugs and closed reduction sites. A gentle taper zone of grafts containing one to three hairs per graft is created, extending posteriorly from the reduced line of plugs. This buffer of smaller grafts softens the transition between the bald nontransplanted posterior scalp and the transplants in the crown-vertex area. The role of finasteride in patients undergoing corrective cannot be overemphasized. These patients already have a donor shortage in the face of ongoing hair loss. Their precious donor supply needs to be used primarily for the corrective process. In addition, some patients who have had donor harvest in high occipital areas are at risk for exposure of the donor scars with progressive hair loss. The administration of finasteride is currently the best option for addressing the problems of progressive hair loss. Correcting previous hair transplantation results that are less than ideal because of the use of poorly performed or outdated techniques is exceedingly gratifying. Patients need to be aware that the process usually takes 2 years and several procedures to complete; however, successful or even partial correction of an unsightly hair restoration procedure is enormously rewarding for the patient. Restoration of the poor hair transplant result is restoration of one s self-esteem and a life-enhancing procedure. The reader should look back at the clinical examples and notice the expression in the postoperative patients eyes to appreciate the truth of this statement. References [1] Vogel JE. Advances in hair restoration surgery. Plast Reconstr Surg 1997;100: [2] Bernstein RM, Rassman WR. Follicular transplantation. Int J Aesthetic Rest Surg 1995;3:119. [3] Bernstein RM, Rassman WR. Aesthetics of follicular transplantation. Dermatol Surg 1997;23:785. [4] Limmer BL. The density issue in hair transplantation. Dermatol Surg 1997;23:747. [5] Orentreich N. Autografts in alopecias and other selected conditions. Ann NY Acad Sci 1959;83:463. [6] Unger WP. Hair transplantation. 3rd edition. New York: Marcel Dekker; [7] Stough DB. Hair replacement. 1st edition. St. Louis (MO): Mosby; [8] Lucas MWG. Partial retransplantation. a new approach in hair transplantation. J Dermatol Surg Oncol 1994; 20:511. [9] Vogel JE. Correction of the cornrow hair transplant and other common problems in surgical hair restoration. Plast Reconstr Surg 2000;105:4. [10] Brandy DA. Techniques for the refinement of abrupt hairlines and donor scars secondary to obsolete punch hair grafting and flaps. Am J Cos Surg 1995;12:4. [11] Epstein J. Revision surgical hair restoration: repair of undesirable results. Plast Reconstr Surg 1999;104:1. [12] Bernstein RM. The art of repair in surgical hair restoration part II: the tactics of repair. Dermatol Surg 2002;28:10. [13] Brandy D. Corrective hair restoration techniques for the aesthetic problems of temperoparietal flaps. Dermatol Surg 2003;29:3. [14] Marzola M. A new alopecia reduction design: no visible scars, no slots, no frechet flaps. Am J Cosmetic Surg 1997;2:167.
Hasson & Wong Lateral Slit Technique in Hair Transplantation Natural hair transplant results, minimized scarring
 Hasson & Wong Lateral Slit Technique in Hair Transplantation Natural hair transplant results, minimized scarring The evolution of follicular unit hair transplants, which involves transplanting hair in
Hasson & Wong Lateral Slit Technique in Hair Transplantation Natural hair transplant results, minimized scarring The evolution of follicular unit hair transplants, which involves transplanting hair in
By the early 1990s, some hair restoration surgeons had began to
 12 Follicular Unit Micrografting By the early 1990s, some hair restoration surgeons had began to regularly cut full size hair transplant grafts into quarters to form minigrafts having three to five hairs
12 Follicular Unit Micrografting By the early 1990s, some hair restoration surgeons had began to regularly cut full size hair transplant grafts into quarters to form minigrafts having three to five hairs
12 Follicular Unit Transplantation
 In: Haber RS, Stough DB, editors: Hair Transplantation, Chapter 12. Elsevier Saunders, 2006: 91-97. 2006, Elsevier Inc. 12 Follicular Unit Transplantation Robert M. Bernstein and William R. Rassman Introduction
In: Haber RS, Stough DB, editors: Hair Transplantation, Chapter 12. Elsevier Saunders, 2006: 91-97. 2006, Elsevier Inc. 12 Follicular Unit Transplantation Robert M. Bernstein and William R. Rassman Introduction
The Art of Repair in Surgical Hair Restoration Part II: The Tactics of Repair
 This is the second part of a two-part series. Part I covered the most common problems encountered in surgical hair restoration and presented general concepts in corrective work. Part II addresses the technical
This is the second part of a two-part series. Part I covered the most common problems encountered in surgical hair restoration and presented general concepts in corrective work. Part II addresses the technical
Understanding Hair Loss and the ARTAS Robotic Procedure
 Understanding Hair Loss and the ARTAS Robotic Procedure THE WORLD'S ONLY ROBOTIC HAIR RESTORATION PROCEDURE * I prefer the ARTAS Robotic Procedure to strip excision surgery. -Vincent, Actual Patient Post
Understanding Hair Loss and the ARTAS Robotic Procedure THE WORLD'S ONLY ROBOTIC HAIR RESTORATION PROCEDURE * I prefer the ARTAS Robotic Procedure to strip excision surgery. -Vincent, Actual Patient Post
Scar Revision and Skin Surgery
 Scar Revision and Skin Surgery Note: Prior to reading this section you should have read Parts I and II of this book! Some scars can be improved with carefully planned multi staged surgery over a period
Scar Revision and Skin Surgery Note: Prior to reading this section you should have read Parts I and II of this book! Some scars can be improved with carefully planned multi staged surgery over a period
WHAT YOU MUST KNOW BEFORE GETTING A HAIR TRANSPLANT ONLINE ENQUIRY
 WHAT YOU MUST KNOW GETTING A HAIR TRANSPLANT 1800 689 939 ONLINE ENQUIRY HAIR LOSS FACTS A full and healthy head of hair is something we take for granted in our youth. A healthy head of hair is a strong
WHAT YOU MUST KNOW GETTING A HAIR TRANSPLANT 1800 689 939 ONLINE ENQUIRY HAIR LOSS FACTS A full and healthy head of hair is something we take for granted in our youth. A healthy head of hair is a strong
Interesting Case Series. Hair Braiding-Induced Scalp Necrosis: A Case Report
 Interesting Case Series Hair Braiding-Induced Scalp Necrosis: A Case Report Zachary Borab, MD, a Madeleine Gantz, MD, a Michael Mirmanesh, MD b and Hengli Lin, MD c a Drexel University College of Medicine,
Interesting Case Series Hair Braiding-Induced Scalp Necrosis: A Case Report Zachary Borab, MD, a Madeleine Gantz, MD, a Michael Mirmanesh, MD b and Hengli Lin, MD c a Drexel University College of Medicine,
Masking the Close Eye Appearance in the East Asian Female Population: Infratemporal Hairline Reduction with Hair Grafting
 Aesth Plast Surg (2016) 40:921 925 DOI 10.1007/s00266-016-0695-9 CASE REPORT COSMETIC MEDICINE Masking the Close Eye Appearance in the East Asian Female Population: Infratemporal Hairline Reduction with
Aesth Plast Surg (2016) 40:921 925 DOI 10.1007/s00266-016-0695-9 CASE REPORT COSMETIC MEDICINE Masking the Close Eye Appearance in the East Asian Female Population: Infratemporal Hairline Reduction with
Aesthetics in Hair Restoration Surgery Feriduni Bijan, MD
 Aesthetics in Hair Restoration Surgery Feriduni Bijan, MD Techniques in hair transplantation In Follicular Unit Transplantation, follicular units can be extracted through two different techniques: Through
Aesthetics in Hair Restoration Surgery Feriduni Bijan, MD Techniques in hair transplantation In Follicular Unit Transplantation, follicular units can be extracted through two different techniques: Through
9 th Annual Hair Transplant 360 Workshop Comprehensive Hair Transplant Course & FUE Hands-On Course Physician s Schedule
 McCulloch Thursday, November 16, 2017 6:45 am SIGN-IN and BREAKFAST 7:00 am Laboratory Guidelines & Safety/ISHRS Introduction 7:15 am Scalp Anatomy Relevant for Every Hair Surgeon/Principles of Hair Transplantation
McCulloch Thursday, November 16, 2017 6:45 am SIGN-IN and BREAKFAST 7:00 am Laboratory Guidelines & Safety/ISHRS Introduction 7:15 am Scalp Anatomy Relevant for Every Hair Surgeon/Principles of Hair Transplantation
Clinical studies with patients have been carried out on this subject of graft survival and out of body time. They are:
 Study Initial Date: July 21, 2016 Data Collection Period: Upon CPHS Approval to September 30, 2018 Study Protocol: Comparison of Out of Body Time of Grafts with the Overall Survival Rates using FUE Lead
Study Initial Date: July 21, 2016 Data Collection Period: Upon CPHS Approval to September 30, 2018 Study Protocol: Comparison of Out of Body Time of Grafts with the Overall Survival Rates using FUE Lead
Enhancing your appearance with a facelift
 PROCEDURE FACT SHEET PLASTIC SURGERY FACELIFT This is a guide for people who are considering a facelift surgery. We advise that you talk to a plastic surgeon and only use this information as a guide to
PROCEDURE FACT SHEET PLASTIC SURGERY FACELIFT This is a guide for people who are considering a facelift surgery. We advise that you talk to a plastic surgeon and only use this information as a guide to
Natural appearance and increased
 Orientation of Multi-Hair Follicles in Nonbald Men: Perpendicular Versus Parallel KUNIYOSHI YAGYU, MD, KOKI HAYASHI, MD, AND STEVEN C. CHANG, MD y BACKGROUND There has been much debate about the orientation
Orientation of Multi-Hair Follicles in Nonbald Men: Perpendicular Versus Parallel KUNIYOSHI YAGYU, MD, KOKI HAYASHI, MD, AND STEVEN C. CHANG, MD y BACKGROUND There has been much debate about the orientation
The hair industry reflects a huge industry in products
 Original Article Cosmetic Combining Follicular Unit Extraction and Scalp Micropigmentation for the Cosmetic Treatment of Alopecias William Rassman, MD Jae Pak, MD Jino Kim, MD Abstract: Two relatively
Original Article Cosmetic Combining Follicular Unit Extraction and Scalp Micropigmentation for the Cosmetic Treatment of Alopecias William Rassman, MD Jae Pak, MD Jino Kim, MD Abstract: Two relatively
Understanding Hair Loss and the ARTAS Robotic Hair Transplant
 Understanding Hair Loss and the ARTAS Robotic Hair Transplant The ARTAS Robotic System Table of Contents PART 1: Understanding Hair Loss 5 6 7 Why am I losing my hair? Why is my hair thinning? How far
Understanding Hair Loss and the ARTAS Robotic Hair Transplant The ARTAS Robotic System Table of Contents PART 1: Understanding Hair Loss 5 6 7 Why am I losing my hair? Why is my hair thinning? How far
9 th Annual Hair Transplant 360 Workshop Comprehensive Hair Transplant Course & FUE Hands-On Course Physician s Schedule November 17-19, 2017
 McCulloch Friday, November 17, 2017 6:45 am SIGN-IN and BREAKFAST 7:00 am Laboratory Guidelines & Safety/ISHRS Introduction S. Lam 7:15 am Scalp Anatomy Relevant for Every Hair Surgeon/Principles of Hair
McCulloch Friday, November 17, 2017 6:45 am SIGN-IN and BREAKFAST 7:00 am Laboratory Guidelines & Safety/ISHRS Introduction S. Lam 7:15 am Scalp Anatomy Relevant for Every Hair Surgeon/Principles of Hair
SCALP ALLURE Motor City Drive Suite 600, Bethesda, MD
 411 Motor City Drive Suite 600, Bethesda, MD 20817 E: daniel@scalpallure.com P: 240-491-7047 W: www.scalpallure.com CORPORATE PROFILE Hair Clinic Providing Scalp Micropigmentation 5,000 5 100% Successful
411 Motor City Drive Suite 600, Bethesda, MD 20817 E: daniel@scalpallure.com P: 240-491-7047 W: www.scalpallure.com CORPORATE PROFILE Hair Clinic Providing Scalp Micropigmentation 5,000 5 100% Successful
PERMANENT HAIR LOSS SOLUTION HAIR TRANSPLANTS
 PERMANENT HAIR LOSS SOLUTION HAIR TRANSPLANTS WHAT IS A HAIR TRANSPLANT? At Hair Transplants Melbourne we move your hair follicles from one area of the scalp (the safe zone) to another area. The safe zone
PERMANENT HAIR LOSS SOLUTION HAIR TRANSPLANTS WHAT IS A HAIR TRANSPLANT? At Hair Transplants Melbourne we move your hair follicles from one area of the scalp (the safe zone) to another area. The safe zone
Corset. Body Lift. The. Operative Step-by-Step Procedure by Alexander P. Moya, M.D. Lewisburg, PA
 The Corset Body Lift Operative Step-by-Step Procedure by Alexander P. Moya, M.D. Lewisburg, PA For more information visit: www.thecorsetbodylift.com About the Author Over the past several years, I have
The Corset Body Lift Operative Step-by-Step Procedure by Alexander P. Moya, M.D. Lewisburg, PA For more information visit: www.thecorsetbodylift.com About the Author Over the past several years, I have
The Face Lift Operation: Foreheads, Cheeks and Necks
 The Face Lift Operation: Foreheads, Cheeks and Necks Note: Prior to reading this section, you should have read Parts I and II and afterwards, read the other Sections in Chapter 4. The Greek word for wrinkle
The Face Lift Operation: Foreheads, Cheeks and Necks Note: Prior to reading this section, you should have read Parts I and II and afterwards, read the other Sections in Chapter 4. The Greek word for wrinkle
Offices in Miami, NYC, Los Angeles, Boca Raton, Aventura, Scottsdale, Tampa, and Naples (FL)
") From the Desk of Jeffrey S. Epstein, MD, FACS MIAMI NEW YORK CITY BOCA RATON Once a year I like to take the opportunity to update my patients and colleagues on news about my practice and the fields of
From the Desk of Jeffrey S. Epstein, MD, FACS MIAMI NEW YORK CITY BOCA RATON Once a year I like to take the opportunity to update my patients and colleagues on news about my practice and the fields of
the bald forehead to the area of central density. (Fig.-2)
") IN PRINCIPLES & TECHNIQUES USED TO CREATE A NATURAL HAIRLINE SURGICAL HAIR RESTORATION Ronald Shapiro Md, Facial Plastic Surgery Clinics of North America, 2004, Volume 12, Number 2 :201-218 1 INTRODUCTION
IN PRINCIPLES & TECHNIQUES USED TO CREATE A NATURAL HAIRLINE SURGICAL HAIR RESTORATION Ronald Shapiro Md, Facial Plastic Surgery Clinics of North America, 2004, Volume 12, Number 2 :201-218 1 INTRODUCTION
Rejuvenation of Myself
 Rejuvenation of Myself Katsuya Takasu, M.D. Nagoya, Japan Face Lift My forehead has deep wrinkles. The jaw is sagging. I have a double chin. The cheeks are also sagging. What can I do to improve my facial
Rejuvenation of Myself Katsuya Takasu, M.D. Nagoya, Japan Face Lift My forehead has deep wrinkles. The jaw is sagging. I have a double chin. The cheeks are also sagging. What can I do to improve my facial
Nipple areola reconstruction
 Nipple areola reconstruction Exceptional healthcare, personally delivered A Brief Outline for Patients following Breast Reconstructive Surgery Introduction Nipple reconstruction is the final stage following
Nipple areola reconstruction Exceptional healthcare, personally delivered A Brief Outline for Patients following Breast Reconstructive Surgery Introduction Nipple reconstruction is the final stage following
RECONSTRUCTION OF THE NOSE AND FOREHEAD BY MEANS OF REGIONAL /ESTHETIC UNITS
 RECONSTRUCTION OF THE NOSE AND FOREHEAD BY MEANS OF REGIONAL /ESTHETIC UNITS By MARIO GONZALEZ-ULLOA, M.D., F.A.C.S., and EDUARDO STEVENS, M.D. Sanatorio Dalinde, Mexico IN this paper we present a case
RECONSTRUCTION OF THE NOSE AND FOREHEAD BY MEANS OF REGIONAL /ESTHETIC UNITS By MARIO GONZALEZ-ULLOA, M.D., F.A.C.S., and EDUARDO STEVENS, M.D. Sanatorio Dalinde, Mexico IN this paper we present a case
Scientific Forum. Minimal Incision Rhytidectomy (Short Scar Face Lift) with Lateral SMASectomy: Evolution and Application
 with Lateral SMASectomy: Evolution and Application") (Short Scar Face Lift) with Lateral SMASectomy: Evolution and Application Daniel C. Baker, MD Background: The evolution of the author s technique for minimal incision rhytidectomy is reviewed. Objective:
(Short Scar Face Lift) with Lateral SMASectomy: Evolution and Application Daniel C. Baker, MD Background: The evolution of the author s technique for minimal incision rhytidectomy is reviewed. Objective:
BREAST RECONSTRUCTION
 BREAST RECONSTRUCTION YOUR OPTIONS FOR BREAST RECONSTRUCTION SURGERY The decision to pursue breast reconstruction is personal and your options vary based on your personal and medical history. This resource
BREAST RECONSTRUCTION YOUR OPTIONS FOR BREAST RECONSTRUCTION SURGERY The decision to pursue breast reconstruction is personal and your options vary based on your personal and medical history. This resource
10 th Annual Hair Transplant 360 Workshop Comprehensive Hair Transplant Course & FUE Hands-On Course Physician s Schedule
 McCulloch Friday, August 3, 2018 6:45 am SIGN-IN and BREAKFAST 7:00 am Laboratory Guidelines & Safety/ISHRS Introduction S. Lam 7:15 am HAIR BASICS Scalp Anatomy Relevant for Every Hair Surgeon S. Wasserbauer
McCulloch Friday, August 3, 2018 6:45 am SIGN-IN and BREAKFAST 7:00 am Laboratory Guidelines & Safety/ISHRS Introduction S. Lam 7:15 am HAIR BASICS Scalp Anatomy Relevant for Every Hair Surgeon S. Wasserbauer
FUE (Follicular Unit Extraction) growth natural appearance painless
 growth natural appearance painless") The Pantovčak Polyclinic - Hair Clinic was founded in 2005 and is the only surgery polyclinic in Croatia and in the region specializing in hair transplantation procedures and treatment of hair loss. All
The Pantovčak Polyclinic - Hair Clinic was founded in 2005 and is the only surgery polyclinic in Croatia and in the region specializing in hair transplantation procedures and treatment of hair loss. All
PROGRAM OUTLINE. As of Jan 17, 2018
 mart PROGRAM OUTLINE As of Jan 17, 2018 Thursday/March 8, 2018 Throughout Day WLSW Arrivals to Dubai 12:00PM-2:00PM Registration and Welcome Lunch 2:00PM-6:00PM Basics Principles Brush Up Your Knowledge
mart PROGRAM OUTLINE As of Jan 17, 2018 Thursday/March 8, 2018 Throughout Day WLSW Arrivals to Dubai 12:00PM-2:00PM Registration and Welcome Lunch 2:00PM-6:00PM Basics Principles Brush Up Your Knowledge
direct brow lift Lift your spirits procedure using the fixation device
 direct brow lift procedure using the fixation device Lift your spirits What is upper eyelid rejuvenation? In general, aging around the eyes is exhibited in two areas: The eye lids and the eyebrows. The
direct brow lift procedure using the fixation device Lift your spirits What is upper eyelid rejuvenation? In general, aging around the eyes is exhibited in two areas: The eye lids and the eyebrows. The
Foreheadplasty. Multimedia Health Education. Disclaimer
 Disclaimer This movie is an educational resource only and should not be used to make a decision on or any facial surgery. All decisions about or any facial surgery must be made in conjunction with your
Disclaimer This movie is an educational resource only and should not be used to make a decision on or any facial surgery. All decisions about or any facial surgery must be made in conjunction with your
Follicular Unit Transplantation 2005
 Dermatologic Clinics 2005; 23(3): 393-414. Issue on Advanced Cosmetic Surgery 2005 by Elsevier Inc. Follicular Unit Transplantation 2005 Robert M. Bernstein, MD,* and William R. Rassman, MD * Associate
Dermatologic Clinics 2005; 23(3): 393-414. Issue on Advanced Cosmetic Surgery 2005 by Elsevier Inc. Follicular Unit Transplantation 2005 Robert M. Bernstein, MD,* and William R. Rassman, MD * Associate
ACCEPTABLE OPERATIVE REPORT # 2
 ACCEPTABLE OPERATIVE REPORT # 2 This operative report follows the standards set by the JCAHO and AAAHC for sufficient information to: identify the patient support the diagnosis justify the treatment document
ACCEPTABLE OPERATIVE REPORT # 2 This operative report follows the standards set by the JCAHO and AAAHC for sufficient information to: identify the patient support the diagnosis justify the treatment document
Cosmetic treatments for hair loss only affect the user s appearance,
 7Cosmetic Treatments Cosmetic treatments for hair loss only affect the user s appearance, and not the structure or function of the living cells that make up the body. Cosmetic hair loss treatments are
7Cosmetic Treatments Cosmetic treatments for hair loss only affect the user s appearance, and not the structure or function of the living cells that make up the body. Cosmetic hair loss treatments are
Surgical creation of a Cupid s bow using W-plasty in patients after cleft lip surgery
 The British Association of Plastic Surgeons (2003) 56, 375 379 Surgical creation of a Cupid s bow using W-plasty in patients after cleft lip surgery Ayako Takeshita*, Tatsuo Nakajima, Tsuyoshi Kaneko,
The British Association of Plastic Surgeons (2003) 56, 375 379 Surgical creation of a Cupid s bow using W-plasty in patients after cleft lip surgery Ayako Takeshita*, Tatsuo Nakajima, Tsuyoshi Kaneko,
Male Pattern Balding. About 30 % of men by age 30 and 50 % by age 50 years of age will have androgenetic alopecia or male pattern balding.
 750 West Broadway Suite 905 - Vancouver BC V5Z 1H8 Phone: 604.283.9299 Fax: 604.648.9003 Email: vancouveroffice@donovanmedical.com Web: www.donovanmedical.com Male Pattern Balding How common is Male Pattern
750 West Broadway Suite 905 - Vancouver BC V5Z 1H8 Phone: 604.283.9299 Fax: 604.648.9003 Email: vancouveroffice@donovanmedical.com Web: www.donovanmedical.com Male Pattern Balding How common is Male Pattern
RUBENHAIR BALTICS Hair transplant and skin health clinic Republikas laukums 3, LV-1010 Riga, Latvia
 RUBENHAIR BALTICS Hair transplant and skin health clinic Republikas laukums 3, LV-1010 Riga, Latvia e-mail: info@rubenhair.eu, phone: +371 Hair transplant Frequently Asked Questions - FAQ 1. What is a
RUBENHAIR BALTICS Hair transplant and skin health clinic Republikas laukums 3, LV-1010 Riga, Latvia e-mail: info@rubenhair.eu, phone: +371 Hair transplant Frequently Asked Questions - FAQ 1. What is a
Silhouette Sutures for Treatment of Facial Aging: Facial Rejuvenation, Remodeling, and Facial Tissue Support
 Silhouette Sutures for Treatment of Facial Aging: Facial Rejuvenation, Remodeling, and Facial Tissue Support Nicanor Isse, MD KEYWORDS Suspension lift Silhouette lift Thread lift Face During facial aging,
Silhouette Sutures for Treatment of Facial Aging: Facial Rejuvenation, Remodeling, and Facial Tissue Support Nicanor Isse, MD KEYWORDS Suspension lift Silhouette lift Thread lift Face During facial aging,
Cosmetic Surgery: Eyelid Surgery (Blepharoplasty)
") Cosmetic Surgery: Eyelid Surgery (Blepharoplasty) This is a guide for people who are considering an eyelid surgery. We advise that you talk to a plastic surgeon and only use this information as a guide
Cosmetic Surgery: Eyelid Surgery (Blepharoplasty) This is a guide for people who are considering an eyelid surgery. We advise that you talk to a plastic surgeon and only use this information as a guide
Endoscopic Brow Lift Post Op
 Endoscopic Brow Lift Post Op RECOVERY TIMETABLE: Approximate recovery after endoscopic brow lift is as follows: DAY 1: Return home, leave any surgical dressing undisturbed until it is removed in the office.
Endoscopic Brow Lift Post Op RECOVERY TIMETABLE: Approximate recovery after endoscopic brow lift is as follows: DAY 1: Return home, leave any surgical dressing undisturbed until it is removed in the office.
Endoscopic Foreheadplasty
 Disclaimer This movie is an educational resource only and should not be used to make a decision on Endoscopic Foreheadplasty or any facial surgery. All decisions about Endoscopic Foreheadplasty or any
Disclaimer This movie is an educational resource only and should not be used to make a decision on Endoscopic Foreheadplasty or any facial surgery. All decisions about Endoscopic Foreheadplasty or any
Dr. Abbasi Hair Clinic
 Dr. Abbasi Hair Clinic Surgical Treatments 1. Scalp flaps: Transferring a hair bearing part of scalps to the bald area. 2. Reducing the extension of the bald area by surgical methods. 3. Planting artificial
Dr. Abbasi Hair Clinic Surgical Treatments 1. Scalp flaps: Transferring a hair bearing part of scalps to the bald area. 2. Reducing the extension of the bald area by surgical methods. 3. Planting artificial
ASAPS Traveling Professors
 ASAPS Traveling Professors Alfonzo Barrera, MD Houston, TX Term: July 2013 June 2015 Advances in Hair Transplantation for the Treatment of Male Pattern Baldness Hair Transplantation Enhancing Aesthetics
ASAPS Traveling Professors Alfonzo Barrera, MD Houston, TX Term: July 2013 June 2015 Advances in Hair Transplantation for the Treatment of Male Pattern Baldness Hair Transplantation Enhancing Aesthetics
Subbrow Blepharoplasty for Upper Eyelid Rejuvenation in Asians
 Oculoplastic Surgery Subbrow lepharoplasty for Upper Eyelid Rejuvenation in Asians INTERNATIONAL CONTRIUTION Daniel Lee, FRCSEd; and Victor Law, FRCSEd ackground: Classical blepharoplasty removes supratarsal
Oculoplastic Surgery Subbrow lepharoplasty for Upper Eyelid Rejuvenation in Asians INTERNATIONAL CONTRIUTION Daniel Lee, FRCSEd; and Victor Law, FRCSEd ackground: Classical blepharoplasty removes supratarsal
INFORMED CONSENT - TATTOO REMOVAL SURGERY
 INFORMED CONSENT - TATTOO REMOVAL SURGERY 2005 American Society of Plastic Surgeons. Purchasers of the Patient Consultation Resource Book are given a limited license to modify documents contained herein
INFORMED CONSENT - TATTOO REMOVAL SURGERY 2005 American Society of Plastic Surgeons. Purchasers of the Patient Consultation Resource Book are given a limited license to modify documents contained herein
SCALP AVULSIONS : ATTEMPT TO RESTORE HAIR GROWTH. By EMIL MEISTER From Surgical Clinic I, University of Vienna
 SCALP AVULSIONS : ATTEMPT TO RESTORE HAIR GROWTH By EMIL MEISTER From Surgical Clinic I, University of Vienna IN the treatment of avulsions of the scalp the covering of the wound with grafts or flaps is
SCALP AVULSIONS : ATTEMPT TO RESTORE HAIR GROWTH By EMIL MEISTER From Surgical Clinic I, University of Vienna IN the treatment of avulsions of the scalp the covering of the wound with grafts or flaps is
CRISTIANO RONALDO NYMD HAIR LOSS & RESTORATION CENTER SOCCER SUPERSTAR. The SUMMER Issue. LUXURIOUS GETAWAYS Venice, Bimini, Cape Cod, & The Hamptons
 SUMMER DINING The Great Outdoors DESTINATION: MIAMI ASTON MARTIN RESIDENCES Living in luxury SOCCER SUPERSTAR CRISTIANO RONALDO The SUMMER Issue LUXURIOUS GETAWAYS Venice, Bimini, Cape Cod, & The Hamptons
SUMMER DINING The Great Outdoors DESTINATION: MIAMI ASTON MARTIN RESIDENCES Living in luxury SOCCER SUPERSTAR CRISTIANO RONALDO The SUMMER Issue LUXURIOUS GETAWAYS Venice, Bimini, Cape Cod, & The Hamptons
The role of the columellar strut in aesthetic COSMETIC. The Effect of the Columellar Strut Graft on Nasal Tip Position in Primary Rhinoplasty
 COSMETIC The Effect of the Columellar Strut Graft on Nasal Tip Position in Primary Rhinoplasty Rod J. Rohrich, M.D. T. Jonathan Kurkjian, M.D. Ronald E. Hoxworth, M.D. Phillip J. Stephan, M.D. Ali Mojallal,
COSMETIC The Effect of the Columellar Strut Graft on Nasal Tip Position in Primary Rhinoplasty Rod J. Rohrich, M.D. T. Jonathan Kurkjian, M.D. Ronald E. Hoxworth, M.D. Phillip J. Stephan, M.D. Ali Mojallal,
YOUR GUIDE TO EYELID SURGERY
 YOUR GUIDE TO EYELID SURGERY Also known as blepharoplasty, eyelid surgery is performed to tighten and rejuvenate the skin around the eyelids. Eyelid surgery can be used for either upper or lower eyelids;
YOUR GUIDE TO EYELID SURGERY Also known as blepharoplasty, eyelid surgery is performed to tighten and rejuvenate the skin around the eyelids. Eyelid surgery can be used for either upper or lower eyelids;
CONSENT FOR BLEPHAROPLASTY SURGERY
 CONSENT FOR BLEPHAROPLASTY SURGERY Blepharoplasty is the medical term for surgery of the eyelids to remove excess skin, possibly muscle, and/or fat from either the upper or lower eyelids. Usually this
CONSENT FOR BLEPHAROPLASTY SURGERY Blepharoplasty is the medical term for surgery of the eyelids to remove excess skin, possibly muscle, and/or fat from either the upper or lower eyelids. Usually this
Refresh, Renew Rejuvenate Look years younger, with minimum downtime. The Quick-Recovery Facelift
 Refresh, Renew Rejuvenate Look years younger, with minimum downtime. The Quick-Recovery Facelift Discover How Easy Looking Younger Can Be. We have pioneered an exciting new facelift procedure that offers
Refresh, Renew Rejuvenate Look years younger, with minimum downtime. The Quick-Recovery Facelift Discover How Easy Looking Younger Can Be. We have pioneered an exciting new facelift procedure that offers
Correction of Thin Lips: A 17-Year Follow-Up of the Original Technique
 Cosmetic Follow-Up Correction of Thin Lips: A 17-Year Follow-Up of the Original Technique Adi Yoskovitch, M.D., and Nabil Fanous, M.D. Montreal, Canada The demand for lip augmentation in the older population
Cosmetic Follow-Up Correction of Thin Lips: A 17-Year Follow-Up of the Original Technique Adi Yoskovitch, M.D., and Nabil Fanous, M.D. Montreal, Canada The demand for lip augmentation in the older population
A Best Friend s Guide to Breast Augmentation
 A Best Friend s Guide to Breast Augmentation About our practice Dr. Russell Hendrick is a plastic and reconstructive surgeon who specializes in reconstructive and aesthetic surgery of the body, as well
A Best Friend s Guide to Breast Augmentation About our practice Dr. Russell Hendrick is a plastic and reconstructive surgeon who specializes in reconstructive and aesthetic surgery of the body, as well
FACE. Facelift Information
 FACE BREAST BODY SKIN Acne Scar Abdominoplasty Breast Reduction Lift Removal Collagen Injections Breast Augmentation Ear Face Pinning/Reduction Lift Laser Skin Treatments Eyelid Lift Dermabrasion Rhinoplasty
FACE BREAST BODY SKIN Acne Scar Abdominoplasty Breast Reduction Lift Removal Collagen Injections Breast Augmentation Ear Face Pinning/Reduction Lift Laser Skin Treatments Eyelid Lift Dermabrasion Rhinoplasty
THE PERMANENCE OF SCARRING, VISIBILITY AND COSMETIC DEFECT
 THE PERMANENCE OF SCARRING, VISIBILITY AND COSMETIC DEFECT The 13 th edition of the Judicial College Guidelines indicate a number of factors to be taken into consideration in the valuation of facial injuries
THE PERMANENCE OF SCARRING, VISIBILITY AND COSMETIC DEFECT The 13 th edition of the Judicial College Guidelines indicate a number of factors to be taken into consideration in the valuation of facial injuries
Hair Replacement Surgery
 Hair Replacement Surgery Springer Berlin Heidelberg New York Barcelona Budapest Hong Kong London Milan Paris Santa Clara Singapore Tokyo P. Bouhanna J.-C. Dardour Hair Replacement Surgery Textbook and
Hair Replacement Surgery Springer Berlin Heidelberg New York Barcelona Budapest Hong Kong London Milan Paris Santa Clara Singapore Tokyo P. Bouhanna J.-C. Dardour Hair Replacement Surgery Textbook and
SCALP ALLURE SPEC BOOK Motor City Drive Suite 600, Bethesda, MD 20817
 SCALP ALLURE SPEC BOOK 10411 Motor City Drive Suite 600, Bethesda, MD 20817 SCALP ALLURE AWARD WINNING ARTIST (Micropigmentation) MEET DANIEL YERENBURG -----------------------------------------------------------------------------------------------------------------------------------------
SCALP ALLURE SPEC BOOK 10411 Motor City Drive Suite 600, Bethesda, MD 20817 SCALP ALLURE AWARD WINNING ARTIST (Micropigmentation) MEET DANIEL YERENBURG -----------------------------------------------------------------------------------------------------------------------------------------
Making you look good is what we do best.
 st. o be d e tw a wh s i Ma n ki g yo u lo ok o go d See how they changed their lives at www.hairclub.com It s time to meet the new you. 01 Face it. No guy wants to lose his hair. Sure, some of us laugh
st. o be d e tw a wh s i Ma n ki g yo u lo ok o go d See how they changed their lives at www.hairclub.com It s time to meet the new you. 01 Face it. No guy wants to lose his hair. Sure, some of us laugh
Start to End About. Anagen Hair Transplant
 Start to End About Anagen Hair Transplant HAIRLOSS, LEADING TO BALDNESS EFFECTS MILLIONS OF MEN AND WOMEN ACROSS THE WORLD. It makes one look older to his/her age. HAIRLOSS STAGES IN MALE & CAUSES OF HAIRLOSS
Start to End About Anagen Hair Transplant HAIRLOSS, LEADING TO BALDNESS EFFECTS MILLIONS OF MEN AND WOMEN ACROSS THE WORLD. It makes one look older to his/her age. HAIRLOSS STAGES IN MALE & CAUSES OF HAIRLOSS
CLINICAL EVALUATION OF REVIVOGEN TOPICAL FORMULA FOR TREATMENT OF MEN AND WOMEN WITH ANDROGENETIC ALOPECIA. A PILOT STUDY
 CLINICAL EVALUATION OF REVIVOGEN TOPICAL FORMULA FOR TREATMENT OF MEN AND WOMEN WITH ANDROGENETIC ALOPECIA. A PILOT STUDY Alex Khadavi, MD, et al,. Los Angeles, CA USA 2004 Abstract: This study was done
CLINICAL EVALUATION OF REVIVOGEN TOPICAL FORMULA FOR TREATMENT OF MEN AND WOMEN WITH ANDROGENETIC ALOPECIA. A PILOT STUDY Alex Khadavi, MD, et al,. Los Angeles, CA USA 2004 Abstract: This study was done
Alopecia December 2005
 TITLE: Alopecia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: December 7, 2005 RESIDENT PHYSICIAN: Garrett Hauptman, MD FACULTY PHYSICIAN: David C. Teller, MD SERIES EDITORS: Francis
TITLE: Alopecia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: December 7, 2005 RESIDENT PHYSICIAN: Garrett Hauptman, MD FACULTY PHYSICIAN: David C. Teller, MD SERIES EDITORS: Francis
Hair restoration
 How to Treat PULL-OUT SECTION www.australiandoctor.com.au COMPLETE HOW TO TREAT QUIZZES ONLINE www.australiandoctor.com.au/cpd to earn CPD or PDP points. INSIDE Patterned hair loss Medical therapy Hair
How to Treat PULL-OUT SECTION www.australiandoctor.com.au COMPLETE HOW TO TREAT QUIZZES ONLINE www.australiandoctor.com.au/cpd to earn CPD or PDP points. INSIDE Patterned hair loss Medical therapy Hair
13 Hair Transplantation
 13 Hair Transplantation Ron Shapiro Bloomington, Minnesota Valerie D. Callender Mitchellville, Maryland SOCIAL IMPACT OF HAIR LOSS Although there are those who accept hair loss gracefully, for many it
13 Hair Transplantation Ron Shapiro Bloomington, Minnesota Valerie D. Callender Mitchellville, Maryland SOCIAL IMPACT OF HAIR LOSS Although there are those who accept hair loss gracefully, for many it
L SILICONE IMPLANT IN AUGMENTATION RHINOPLASTY FOR THE ASIAN ( 15 years of experience )
") L SILICONE IMPLANT IN AUGMENTATION RHINOPLASTY FOR THE ASIAN ( 15 years of experience ) Speaker : Mr DIEP THE DUNG M.D Specialty : Cosmetic Surgery Clinic : Dr Dung s Beauty Clinic Address : Can Tho city
L SILICONE IMPLANT IN AUGMENTATION RHINOPLASTY FOR THE ASIAN ( 15 years of experience ) Speaker : Mr DIEP THE DUNG M.D Specialty : Cosmetic Surgery Clinic : Dr Dung s Beauty Clinic Address : Can Tho city
DANIEL LANZER COSMETIC SURGEON WITH 25+ YEARS EXPERIENCE
 DR DANIEL LANZER COSMETIC SURGEON WITH 25+ YEARS EXPERIENCE ADVANCED EAR CORRECTIONS WITH DR. RYAN WELLS The latest advanced minimally invasive cosmetic ear correction technique has been introduced to
DR DANIEL LANZER COSMETIC SURGEON WITH 25+ YEARS EXPERIENCE ADVANCED EAR CORRECTIONS WITH DR. RYAN WELLS The latest advanced minimally invasive cosmetic ear correction technique has been introduced to
While you ve been losing your hair, new options. have emerged for getting it back. For men. For women. See what s possible now.
 While you ve been losing your hair, new options have emerged for getting it back. For men. For women. See what s possible now. Of course you hate it that your hair s thinning. The image in the mirror just
While you ve been losing your hair, new options have emerged for getting it back. For men. For women. See what s possible now. Of course you hate it that your hair s thinning. The image in the mirror just
Discussion. Surgical Anatomy of the Ligamentous Attachments of the Lower Lid and Lateral Canthus. Surgical Anatomy of the Midcheek and Malar Mounds
 Discussion Surgical Anatomy of the Ligamentous Attachments of the Lower Lid and Lateral Canthus by Arshad R. Muzaffar, M.D., Bryan C. Mendelson, F.R.C.S.Ed., F.R.A.C.S., F.A.C.S., and William P. Adams,
Discussion Surgical Anatomy of the Ligamentous Attachments of the Lower Lid and Lateral Canthus by Arshad R. Muzaffar, M.D., Bryan C. Mendelson, F.R.C.S.Ed., F.R.A.C.S., F.A.C.S., and William P. Adams,
Our Dermatology Online Original Article
 Our Dermatology Online Original Article A study on scar revision Ashutosh Talwar 1, Neerja Puri 2 1 Department of Surgery, Punjab Health Systems Corporation, Ferozepur, Punjab, India, 2 Department of Dermatology
Our Dermatology Online Original Article A study on scar revision Ashutosh Talwar 1, Neerja Puri 2 1 Department of Surgery, Punjab Health Systems Corporation, Ferozepur, Punjab, India, 2 Department of Dermatology
Welcome to Looks Forever
 Welcome to Looks Forever From times immemorial humans have been obsessed with beauty. The times we live in, place a stronger emphasis on the way we look, our presence. Evolving from our granni e advices
Welcome to Looks Forever From times immemorial humans have been obsessed with beauty. The times we live in, place a stronger emphasis on the way we look, our presence. Evolving from our granni e advices
Please keep in mind that while we can recreate your natural feminine shape, you might have areas of numbness. The
 Vol 1 Issue 1 FALL 2008 Profile Of A Breast Reconstruction When a woman has been diagnosed with breast cancer and the medical decision has been made to remove a breast, she may experience feelings of identity
Vol 1 Issue 1 FALL 2008 Profile Of A Breast Reconstruction When a woman has been diagnosed with breast cancer and the medical decision has been made to remove a breast, she may experience feelings of identity
Alopecia in the Primary Care Setting BETH L. BROGAN, MD
 Alopecia in the Primary Care Setting BETH L. BROGAN, MD Typical Patient Presentation A middle aged woman Anxious and upset regarding hair loss, sometimes holding a bag of hair Has noticed hair loss including
Alopecia in the Primary Care Setting BETH L. BROGAN, MD Typical Patient Presentation A middle aged woman Anxious and upset regarding hair loss, sometimes holding a bag of hair Has noticed hair loss including
HAIR LOSS. Types of Hair Loss
 HAIR LOSS Hair loss is a common condition that affects most people (depending on the severity) at some point in their lives. Humans have between 100,000 and 150,000 strands hairs on their head. The number
HAIR LOSS Hair loss is a common condition that affects most people (depending on the severity) at some point in their lives. Humans have between 100,000 and 150,000 strands hairs on their head. The number
Choices for women thinking about breast reconstruction. EMPOWER SUPPORT ADVOCATE
 Choices for women thinking about breast reconstruction. About breast reconstruction Breast reconstruction is the rebuilding of your breast after a mastectomy due to breast cancer, or the prevention of
Choices for women thinking about breast reconstruction. About breast reconstruction Breast reconstruction is the rebuilding of your breast after a mastectomy due to breast cancer, or the prevention of
CONSUMER GUIDE TO HAIR LOSS AND HAIR TRANSPLANT. dhi-philippines.com (+632)
") CONSUMER GUIDE TO HAIR LOSS AND HAIR TRANSPLANT (+632) 893 6175 Physically, hair plays an important role in protecting our scalp from the sun and helping to maintain body temperature. Emotionally, your
CONSUMER GUIDE TO HAIR LOSS AND HAIR TRANSPLANT (+632) 893 6175 Physically, hair plays an important role in protecting our scalp from the sun and helping to maintain body temperature. Emotionally, your
Electrosurgical Grounding Pads
 Electrosurgical Grounding Pads Manufactured by 3M Medical Division The revolutionary electrosurgical pad that s easy to place because of its smaller size. The Medline Universal Electrosurgical Pad 9100
Electrosurgical Grounding Pads Manufactured by 3M Medical Division The revolutionary electrosurgical pad that s easy to place because of its smaller size. The Medline Universal Electrosurgical Pad 9100
FACETITE: SUBDERMAL RADIOFREQUENCY SKIN TIGHTENING AND FACE CONTOURING
 FACETITE: SUBDERMAL RADIOFREQUENCY SKIN TIGHTENING AND FACE CONTOURING R. Stephen Mulholland, MD, FRCS(C)* and Michael Kreindel, PhD** *Private Plastic Surgery Practice, Toronto, Canada ** Chief Technology
FACETITE: SUBDERMAL RADIOFREQUENCY SKIN TIGHTENING AND FACE CONTOURING R. Stephen Mulholland, MD, FRCS(C)* and Michael Kreindel, PhD** *Private Plastic Surgery Practice, Toronto, Canada ** Chief Technology
Topical skin adhesive products designed for effective wound closure
 Topical skin adhesive products designed for effective wound closure McKesson understands the challenges you face and is dedicated to providing quality, cost-effective solutions. Our exclusive brand of
Topical skin adhesive products designed for effective wound closure McKesson understands the challenges you face and is dedicated to providing quality, cost-effective solutions. Our exclusive brand of
TECHNIQUE FOR PRESERVATION OF THE TEMPORAL BRANCHES OF THE FACIAL NERVE DURING FACE-LIFT OPERATIONS. By RAUL LOEB
 TECHNIQUE FOR PRESERVATION OF THE TEMPORAL BRANCHES OF THE FACIAL NERVE DURING FACE-LIFT OPERATIONS By RAUL LOEB Plastic Surgery Department, Escola PauIista de Medicina, S~o Paulo, Brazil IN general, papers
TECHNIQUE FOR PRESERVATION OF THE TEMPORAL BRANCHES OF THE FACIAL NERVE DURING FACE-LIFT OPERATIONS By RAUL LOEB Plastic Surgery Department, Escola PauIista de Medicina, S~o Paulo, Brazil IN general, papers
How to remove nose skin excess? Aesthetically reasonable approach
 Otorhinolaryngology-Head and Neck Surgery Research Article ISSN: 2398-4937 How to remove nose skin excess? Aesthetically reasonable approach M. Sulamanidze*, G.Sulamanidze, and K. Sulamanidze Clinic of
Otorhinolaryngology-Head and Neck Surgery Research Article ISSN: 2398-4937 How to remove nose skin excess? Aesthetically reasonable approach M. Sulamanidze*, G.Sulamanidze, and K. Sulamanidze Clinic of
Non-Surgical Epicanthoplasty and Rhinoplasty: Epicanthorhinoplasty
 JKAU: Med. Sci., Vol. 17 No. 2, pp: 3-9 (2010 A.D. / 1431 A.H.) DOI: 10.4197/Med. 17-2.1 Non-Surgical Epicanthoplasty and Rhinoplasty: Epicanthorhinoplasty Amal A. Bukhari, MD, FRCS Department of Ophthalmology,
JKAU: Med. Sci., Vol. 17 No. 2, pp: 3-9 (2010 A.D. / 1431 A.H.) DOI: 10.4197/Med. 17-2.1 Non-Surgical Epicanthoplasty and Rhinoplasty: Epicanthorhinoplasty Amal A. Bukhari, MD, FRCS Department of Ophthalmology,
Nasolabial Evaluation of the Unilateral Cleft Lip Repair
 Nasolabial Evaluation of the Unilateral Cleft Lip Repair Luis Bermudez, M.D. There are several reasons to develop a standardized system to measure the surgical results in cleft lip and palate patients:
Nasolabial Evaluation of the Unilateral Cleft Lip Repair Luis Bermudez, M.D. There are several reasons to develop a standardized system to measure the surgical results in cleft lip and palate patients:
Sunetics Clinical Laser Unit
 Clinical Laser Unit Hair loss can often be an undesirable aspect of life. Fortunately, with recent advances in technology, there are several treatments that may reduce, prevent, or even reverse hair loss.
Clinical Laser Unit Hair loss can often be an undesirable aspect of life. Fortunately, with recent advances in technology, there are several treatments that may reduce, prevent, or even reverse hair loss.
INFORMED CONSENT MEDICAL TATTOOING & SKIN TREATMENT
 INFORMED CONSENT MEDICAL TATTOOING & SKIN TREATMENT. Purchasers of the Patient Consultation Resource Book are given a limited license to modify documents contained herein and reproduce the modified version
INFORMED CONSENT MEDICAL TATTOOING & SKIN TREATMENT. Purchasers of the Patient Consultation Resource Book are given a limited license to modify documents contained herein and reproduce the modified version
Face and Neck Lift MedBelle Information Brochure
 Face and Neck Lift MedBelle Information Brochure Why we prepared this brochure for you Hi, my name is Sarah. I m a cosmetic treatment adviser with MedBelle. Every day, I speak with patients in the UK looking
Face and Neck Lift MedBelle Information Brochure Why we prepared this brochure for you Hi, my name is Sarah. I m a cosmetic treatment adviser with MedBelle. Every day, I speak with patients in the UK looking
Lower Blepharoplasty With Direct Excision of Skin Excess: A Five-Year Experience. Pietro Bellinvia, MD, Francesco Klinger, MD, Giacomo Bellinvia, MD
 Lower Blepharoplasty With Direct Excision of Skin Excess: A Five-Year Experience Pietro Bellinvia, MD, Francesco Klinger, MD, Giacomo Bellinvia, MD INTERNATIONAL CONTRIBUTION Oculoplastic Surgery Lower
Lower Blepharoplasty With Direct Excision of Skin Excess: A Five-Year Experience Pietro Bellinvia, MD, Francesco Klinger, MD, Giacomo Bellinvia, MD INTERNATIONAL CONTRIBUTION Oculoplastic Surgery Lower
Invites you to an evening of sharing real survivor stories. Learn from experience and discover your healing options. CELEBRATION
 Invites you to an evening of sharing real survivor stories. Learn from experience and discover your healing options. CELEBRATION Breast Reconstruction Awareness Day CELEBRATE BREAST RECONSTRUCTION AWARENESS
Invites you to an evening of sharing real survivor stories. Learn from experience and discover your healing options. CELEBRATION Breast Reconstruction Awareness Day CELEBRATE BREAST RECONSTRUCTION AWARENESS
Mr Eoin O Broin FRCS (Plast) MD Consultant Plastic and Reconstructive Surgeon TEMPORARY INFORMATION SHEET (WORK IN PROGRESS) BREAST RECONSTRUCTION
 MD Consultant Plastic and Reconstructive Surgeon TEMPORARY INFORMATION SHEET (WORK IN PROGRESS) BREAST RECONSTRUCTION") Mr Eoin O Broin FRCS (Plast) MD Consultant Plastic and Reconstructive Surgeon TEMPORARY INFORMATION SHEET (WORK IN PROGRESS) BREAST RECONSTRUCTION Breast reconstruction involves surgery to replace the
Mr Eoin O Broin FRCS (Plast) MD Consultant Plastic and Reconstructive Surgeon TEMPORARY INFORMATION SHEET (WORK IN PROGRESS) BREAST RECONSTRUCTION Breast reconstruction involves surgery to replace the
BERNSTEIN MEDICAL, P.C.
 BERNSTEIN MEDICAL, P.C. 110 East 55 th Street, 11 th Floor, New York, NY 10022 212-826-2400 contact@bernsteinmedical.com Instructions After Your FUE Procedure Please Note: These instructions have been
BERNSTEIN MEDICAL, P.C. 110 East 55 th Street, 11 th Floor, New York, NY 10022 212-826-2400 contact@bernsteinmedical.com Instructions After Your FUE Procedure Please Note: These instructions have been
Kurt Ortwig NP NorthShore University Health System Department of Emergency Medicine
 Kurt Ortwig NP NorthShore University Health System Department of Emergency Medicine Other types of wound closure Tissue adhesive Metal skin staples Adhesive strips Skin Glue Not Superglue: Honey, I glued
Kurt Ortwig NP NorthShore University Health System Department of Emergency Medicine Other types of wound closure Tissue adhesive Metal skin staples Adhesive strips Skin Glue Not Superglue: Honey, I glued
Advanced Skin Rejuvenation Wrinkle Enhancement and Skin Resurfacing Procedures
 Advanced Skin Rejuvenation Wrinkle Enhancement and Skin Resurfacing Procedures Note: Prior to reading this section, you should have read Parts I and II of this book, in particular, the section beginning
Advanced Skin Rejuvenation Wrinkle Enhancement and Skin Resurfacing Procedures Note: Prior to reading this section, you should have read Parts I and II of this book, in particular, the section beginning
Jeffrey S. Epstein, M.D., FACS. Pre and Post Operative Instructions for FUE Hair Transplants
 Pre and Post Operative Instructions for FUE Hair Transplants Hair restoration is a delicate process and it is important that you understand the nature, goals, potential complications, and limitations of
Pre and Post Operative Instructions for FUE Hair Transplants Hair restoration is a delicate process and it is important that you understand the nature, goals, potential complications, and limitations of
Radiant Skin Dermatology and Laser
 Pre-op Instructions Before Surgery Wash your hair the day before surgery with Hibiclens and your regular shampoo, in a 50/50 ratio, let sit for a minute and then rinse out. Do not wash your hair the day
Pre-op Instructions Before Surgery Wash your hair the day before surgery with Hibiclens and your regular shampoo, in a 50/50 ratio, let sit for a minute and then rinse out. Do not wash your hair the day
Facelift (Rhytidectomy)
") Houston (Rhytidectomy) in (Rhytidectomy) (Rhytidectomy) Houston A (Rhytidectomy) is a common surgery that provides an excellent way to improve facial contours that no longer reflect a patient s youthful
Houston (Rhytidectomy) in (Rhytidectomy) (Rhytidectomy) Houston A (Rhytidectomy) is a common surgery that provides an excellent way to improve facial contours that no longer reflect a patient s youthful
Skin Laxity of the Face and Neck: Treatment Approach with the Titan Device. LISA S. BUNIN, M.D. Allentown, Pennsylvania
 Skin Laxity of the Face and Neck: Treatment Approach with the Titan Device LISA S. BUNIN, M.D. Allentown, Pennsylvania LISA S. BUNIN, M.D., Allentown, Pennsylvania Patients today are becoming accuomed
Skin Laxity of the Face and Neck: Treatment Approach with the Titan Device LISA S. BUNIN, M.D. Allentown, Pennsylvania LISA S. BUNIN, M.D., Allentown, Pennsylvania Patients today are becoming accuomed
Heather Woolery-Lloyd, M.D.
 Heather Woolery-Lloyd, M.D. Director of Ethnic Skin Care Voluntary Assistant Professor Miller/University of Miami School of Medicine Department of Dermatology and Cutaneous Surgery Disclosure of Commercial
Heather Woolery-Lloyd, M.D. Director of Ethnic Skin Care Voluntary Assistant Professor Miller/University of Miami School of Medicine Department of Dermatology and Cutaneous Surgery Disclosure of Commercial
Results of Nipple Reconstruction Using the Modified Double Opposing Tab Flap Technique
 Results of Nipple Reconstruction Using the Modified Double Opposing Tab Flap Technique Khaldoun J. Haddadin MD*, Nasser Q. hmad MD* STRCT Objective: Nipple-areola reconstruction represents the final stage
Results of Nipple Reconstruction Using the Modified Double Opposing Tab Flap Technique Khaldoun J. Haddadin MD*, Nasser Q. hmad MD* STRCT Objective: Nipple-areola reconstruction represents the final stage
THE LIPS ARE AN ESSENTIAL
 Quantitative Analysis of Lip Appearance After V-Y Lip Augmentation Andrew A. Jacono, MD; Vito C. Quatela, MD ORIGINAL ARTICLE Objective: To quantitatively analyze the changes in the 3-dimensional appearance
Quantitative Analysis of Lip Appearance After V-Y Lip Augmentation Andrew A. Jacono, MD; Vito C. Quatela, MD ORIGINAL ARTICLE Objective: To quantitatively analyze the changes in the 3-dimensional appearance